(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A male patient in his 60s with a history of urothelial carcinoma metastatic to the liver, status post radical cystoprostatectomy and chemotherapy. Patient later presented with right renal pelvis tumor. The biopsy showed fragments of high grade urothelial carcinoma with inverted growth pattern, with tumor cells positive for uroplakin II + III, CAM 5.2, and GATA-3 by immunohistochemical analysis. Patient was treated with gemcitabine, carboplatin and Enfortumab but progressed, with evidence of new lung and liver metastases. Oncomine NGS testing was performed to identify potential therapeutic targets.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
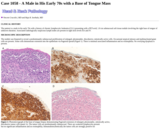
The patient is a male in his early 70s with a history of chronic lymphocytic leukemia (CLL) presenting with a PET-avid, 1.8 cm submucosal soft tissue nodule involving the right base of tongue of unknown duration. Associated radiologically suspicious lymph nodes are present in right neck levels IIA and IV.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
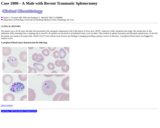
A peripheral blood smear demonstrated the following:
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a man in his 20s with a 5 year history of deafness presenting with edema, nephrotic range proteinuria (urine protein / creatinine ratio of 15.5), mild hypertension (154/81 mm Hg) and severe anemia (hemoglobin-3.3 g/dL, hematocrit-9.7%). The patient had no history of diabetes mellitus, NSAIDs use, drugs or alcohol, or other listed medications and has no evidence of a gastrointestinal bleed. The patient did have a family history of deafness in both his mother and younger brother.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his 30's presented to the emergency department following a tonic-clonic seizure with generalization. He had no history of prior seizures and denied any trauma, vision changes, imbalance, memory issues, weakness or paresthesia. Brain MRI discovered two separate areas of expansile T2 FLAIR hyperintensity, with discrete lesions seen in the left frontal lobe and right medial parietooccipital region. Neither lesion showed enhancement following administration of contrast. A CT scan of the chest, abdomen and pelvis revealed no evidence of primary malignancy. Given the radiological characteristics, multifocal glioma was suspected, with a differential diagnosis of acute disseminated encephalomyelitis and nonenhancing tumefactive multiple sclerosis. The patient subsequently underwent craniotomies for resection of both lesions with a 6-week interval.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in late thirties presented to the Urology clinic with complaint of hematospermia since 6 months.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his forties with a history of basal cell carcinoma of the nose and a benign neoplasm of the jaw, status post resection with mandibular reconstruction, presented for routine follow-up. On chest x-ray workup, he was found to have numerous bilateral pulmonary nodules that were highly suspicious for a metastatic disease. A follow-up CT scan of the chest with contrast showed eight small round pulmonary nodules measuring few millimeters in size and a larger left lower lobe pulmonary mass measuring 3.0 x 3.1 cm in size. There was no evidence of hilar or mediastinal lymphadenopathy and no pleural nodularity or effusion on imaging.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A male in his 50s with a history of bioprosthetic aortic valve replacement and coronary artery bypass graft presented after being found unconscious at home. His blood cultures grew Streptococcus Viridans group and intravenous antibiotics were initiated. A transesophageal echocardiogram showed an aortic valve vegetation and moderate aortic regurgitation without overt findings of an aortic root abscess. Several days later he became acutely short of breath, his mean arterial pressures dropped from about 130 to 40s-50s, and he became bradycardic. Resuscitation efforts began and a repeat transesophageal echocardiogram performed during these efforts showed right sided aortic annular echolucency on the right ventricle/tricuspid valve side of the aortic root with possible fistula formation. Unfortunately he suffered PEA arrest and was pronounced deceased after advanced cardiac life support failed to resuscitate him. A hospital autopsy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A middle aged man was admitted to the neurology service for acute onset aphasia and right sided weakness. He received tPA due to clinical concern for stroke, however, subsequent brain MRI was not consistent with ischemic stroke. Scans showed multiple nonenhancing periventricular and subcortical zones of abnormal T2 signal with associated prior hemorrhage (Figure 1). The leading diagnostic consideration was vasculitis and/or vasculopathy. Other considerations were lymphoma or septic emboli, but CSF and flow cytometry studies were negative and lab values did not support an infectious process. The working diagnosis was inflammatory amyloid angiitis based on clinicoradiological criteria. He was treated with steroids and improved sufficiently for discharge.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a man in his 60s with new detection of hypertension and chronic kidney disease presenting with nephrotic range proteinuria, and peripheral edema. The patient was a former smoker (50 pack years) and had used NSAID (Celebrex and Ibuprofen) for many years for his chronic back pain, but discontinued 3 months prior to kidney biopsy after he was found to have an elevated serum creatinine(Table 1) and additional pertinent labs (Table 2) include:
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his 60's with a history of metastatic lung adenocarcinoma presents with progression of disease identified by positron emission tomography (PET) scan. He was initially diagnosed with lung cancer 4 years prior, when a 5.0 cm left infrahilar mass and left hilar lymphadenopathy was identified. At that time, cytologic evaluation of an endobronchial ultrasound-guided fine needle aspiration of his subcarinal lymph node demonstrated metastatic lung adenocarcinoma (Figure 1). Next-generation sequencing of the tumor using an oncologic hotspot panel identified an EGFR exon 19 deletion (p.E746_A750del), but no other mutations. Fluorescence in-situ hybridization studies (FISH) did not identify ALK rearrangement, ROS1 translocation, RET translocation, or MET amplification. Immunohistochemistry showed PD-L1 was expressed on 1% of the malignant cells. The tumor was classified as unresectable stage IIIC lung adenocarcinoma, cT3 N3.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his late 30's with a medical history of HIV, hypertension and chronic kidney disease presented with acute kidney Injury and positivity for COVID-19 infection. He was on anti-HIV medication (cobicistat-darunavir).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A male patient in the sixties, presented with an itchy 1.0 x 1.0 cm blue-black dome-shaped nodule over the left preauricular cheek with superficial erosion for 3 years (Figure 1). No family history of dysplastic nevi or melanoma was noted. The specimen was an excisional biopsy, measuring 1.8 x 1.3 x 1.1 cm that was serially sectioned.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his late 60s presented with low appetite and early satiety symptoms since 2-3 weeks. Weight loss of more than 20kg was also noted in the past year. The patient also had a worsening generalized pruritis and diffuse body rash for 4-6 months. He was initially treated for scabies but the pruritis and rash did not resolve. Axillary, subcarinal, mediastinal, retroperitoneal, pelvic and inguinal lymphadenopathy was found on CT imaging. The largest node was left axillary lymph node which measured 1.7 cm while rest of the abdominal and the mediastinal lymph nodes had a maximum diameter of 1.2-1.3 cm. Due to the lymphadenopathy, constitutional symptoms, significant weight loss and history of rash, lymphoma was the major consideration. The patient's past medical history was significant for chronic kidney disease, COPD and hypertension. A diagnosis of MGUS was made 3 years ago but the bone marrow was not involved by a plasma cell neoplasm. The abnormal protein detected on serum protein electrophoresis (SPEP) was 0.3 g/dl at that time and immunofixation revealed IgG Kappa monoclonal gammopathy and monoclonal free lambda light chain. The free kappa to lambda light chain ratio was 0.89.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A middle aged male with an abnormal digital rectal exam with imaging consistent with a seminal vesicle mass. The most recent serum PSA level was 0.75 ng/mL. Due to clinical suspicion about the mass originating from the prostate gland, the patient underwent a core needle biopsy procedure. Core fragments were received from the patient and were labeled as 'prostatic tissue' which showed a malignant spindle cell neoplasm with focal staining for cytokeratin AE1/AE3, with a morphologic differential diagnosis which included carcinosarcoma and high-grade sarcoma (prostatic stromal sarcoma, solitary fibrous tumor with high-grade sarcomatous transformation). Due to paucity of tissue, further classification was not possible and therefore the patient underwent a radical prostatectomy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The neonate was the product of an uneventful 39-4/7 week pregnancy with normal delivery and adequate initial Apgar scores. Soon after birth, the neonate developed cyanosis, left side pneumothorax and lung parenchymal abnormalities with opacity on x-ray. He expired at 12 days of age in the setting of progressive respiratory failure, pulmonary hypertension, and finally acute kidney failure. An autopsy revealed normal cardiac anatomy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 3-day-old male newborn was brought to the outside hospital (OSH) emergency department by his mother with complaints of poor feeding, lethargy, and excessive sleep.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Police and EMS were called to the scene of a man in his mid-twenties with a past medical history of ADHD. At the scene, the patient was found to be extremely agitated with altered mental status. He was shot multiple times with tasers by the police in order to be subdued.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Female patient in her 60's presented to an outside hospital with a "lump" in her medial thigh. Outside providers thought the lesion to be a hematoma though the patient was not on anticoagulants or recalled any trauma to that area. The lesion did not resolve after some time. Upon excision, the "lump" was discovered to be a tumor. The patient was referred to our hospital system for radical re-excision of the lesion along with lymph node dissection. Pathologic evaluation demonstrated the tumor to be composed of sheets of pleomorphic epithelioid cells with abundant amphophilic cytoplasm and marked nuclear pleomorphism with frequent mitotic figures (see below). The lymph node was positive for metastatic tumor. Immunohistochemistry demonstrated the tumor cells to be negative for PANCK, CK5/6, p40, S100, SOX10, Melan-A, HMB45, SMA, desmin, CD34, and ERG with rare cells positive for p40. A preliminary diagnosis of undifferentiated pleomorphic sarcoma was rendered. However, since sarcomas usually do not metastasize through the lymphatic system the tumor was submitted for molecular testing.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
68 year old woman presented with a swollen and tender mass in her left breast. The patient has a history of fibrocystic changes with cyst formation. Diagnostic mammogram and ultrasound showed a 4.8 x 4.8 x 2.7 cm solid and cystic mass with irregular borders and mixed echogenicity located against the chest wall at the 6:00 position approximately 6 cm from the nipple (see below). Core needle biopsy was performed, demonstrating the histopathology shown below, and ER/PR/HER2 immunohistochemistry demonstrated a triple negative phenotype. The patient was evaluated for neoadjuvant therapy and none was performed after proper pathologic diagnosis. The patient then underwent left breast lumpectomy with sentinel lymph node biopsy (see below).
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.