(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a young male child with no significant past medical history presented with fever and sore throat. His complete blood count findings are shown in the table.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An elderly, Caucasian, postmenopausal female presented for her annual gynecological examination. Her main complaint was a three day history of rectal pressure, one month prior to presentation. Significantly, her previous pap smear (two years ago) was negative for intraepithelial lesion or malignancy. She denied having any abdominal pain or distension, early satiety, change in bowel or bladder habits, and no vaginal symptoms. On bimanual examination, she was noted to have a posterior uterine mass. Subsequent pelvic ultrasound revealed a thickened endometrial lining of 21.2mm, and a complex left adnexal, solid cystic mass measuring 13.9x7.3x10.5cm with thick/thin septations and a solid component with vascular flow. An elective left salpingo-oophorectomy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
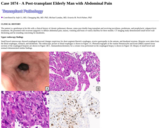
A postmenopausal woman in her 70s presented to the emergency room with abdominal pain. Physical examination revealed a non-mobile, non-tender right pelvic mass. Ultrasound found a large right ovarian mass, measuring about 9.2 x 7.6 x 7.2 cm. CA-125 was elevated at 42 (ref 0-20). Her past medical history was not contributory. The patient reported neither vaginal bleeding nor discharge. A total abdominal hysterectomy, bilateral salpingo-oophorectomy, lymphadenectomy and omentectomy were performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Immunodeficient individuals in general are prone to various infections, including viral. In the setting of acquired or congenital immunodeficiency, certain viruses are associated with specific tumors such as HHV8 associated Kaposi sarcoma and EBV-associated post-transplant lymphoproliferative diseases (PTLD) (Hussein, Rath, Ludewig, Kreipe, & Jonigk, 2014). A rare and lesser known entity is immunodeficiency associated smooth muscle tumors. In 1970 Pritzker et al described a smooth muscle tumor of the bowel metastatic to the liver in an immunosuppressed patient, later on Chadwick et al associated smooth muscle tumors with AIDS in three children (Chadwick, 1990; Pritzker, Huang, & Marshall, 1970). In 1995 the association between EBV and smooth muscle tumors was described in immunosuppressed patients following organ transplantation and in children with AIDS (Lee et al., 1995; McClain et al., 1995).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
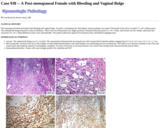
Post-menopausal female presented with bleeding and vaginal bulge. On pelvic examination her third degree uterine prolapse was noted. Ultrasound of the pelvis revealed 71 x 44 x 44mm uterus. The endometrial lining measured 4.3mm in thickness. There were two leiomyomas one, Right, posterior, intramural that measured 13 x 14 x 13mm. and second was left, fundal, subserosal that measured 16 x 16 x 14mm.Bilateral ovaries were unremarkable. The patient underwent supracervical hysterectomy and bilateral salpingectomy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a gentleman in his 60s with a clinical history of chronic pulmonary disease, status post double lung transplant and receiving tacrolimus, prednisone, and prophylactic valganciclovir treatments. He presented with recurrent epigastric to diffuse abdominal pain, nausea, vomiting and bouts of watery diarrhea for three months. CT imaging study demonstrated small bowel wall thickening and fat stranding concerning for duodenitis.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a preadolescent female who presented with nausea, vomiting, blurred vision, diplopia, gait instability and ataxia. An MRI showed a 22 x 21 x 78 mm enhancing tumor with a necrotic center located at the craniocervical junction expanding the medulla oblongata and the proximal aspect of the spinal cord to the level of T3. Additionally, there was a non-enhancing exophytic component of the tumor abutting the left premedullary cistern (Figure 1). The radiologic impression was an infiltrative, likely astrocytic, craniocervical junction tumor with an exophytic component.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a premature infant male who was born to a multiparous mother. Early in the mother's pregnancy, routine prenatal screening identified fetal anemia requiring multiple percutaneous umbilical blood sampling (PUBS) procedures and fetal transfusions. A workup for immune mediated causes of fetal anemia was completely negative. During one PUBS procedure, the fetus showed a significant cardiac deceleration, leading to an emergent C-section. His immediate post-delivery course was complicated by multiple prematurity associated comorbidities, as well as unexplained persistent anemia without reticulocytosis requiring transfusion support. Hematology was consulted for the persistent anemia and recommended a bone marrow aspirate and biopsy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A teenage female presented with secondary amenorrhea. The patient had 1 menstrual cycle 3 years ago and has had no menses since. Laboratory work-up was negative for pregnancy test, mildly increased calcium level (11.7 mg/dL, normal range: 8.5-10.2 mg/dL) and CA 125 (43 Units/ml, normal range: 0-20 Units/ml). Prolactin, TSH, AFP, Inhibin A, Inhibin B and CEA were normal. Imaging revealed a 13 x 11.8 x 8.6 cm, predominately cystic left pelvis mass, with multiple internal septations. Her past medical history was not contributory. Patient underwent left salpingo-oophorectomy, omentectomy and tumor debulking with intraoperative frozen section consultation.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A teenage girl presented to an outside facility due to headache. Her symptoms started approximately about a month and a half prior to presentation, initially being just a headache but had progressed with the patient developing nausea and vomiting. She subsequently underwent an MRI which showed a 3.5 x 3.2 cm mass lesion, with a low signal on T1 and a high signal on T2-weighted images, demonstrating a nodular thick rind of enhancement and marked surrounding vasogenic edema. The patient was taken to the operating room for resection and a 2.5 x 1.1 x 0.2 cm aggregate of tan-white to tan-red, glistening, hemorrhagic soft to rubbery tissue was received for evaluation.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was an otherwise healthy girl, who first noted the lump approximately two years ago without any significant change over time. There was no apparent history of trauma and no apparent history of intercurrent illness at that stage. No associated redness, discharge or skin changes were noted. The mass became slightly tender, especially to palpation. She denied the presence of additional masses anywhere else. On physical examination, a single mass was palpated in the upper anterior triangle to the left of the midline, approximately 2-3 cm under the mandible and above and lateral to the thyroid and cricothyroid cartilage. The mass did not move with tongue protrusion. The lump itself was approximately 8 mm in diameter, felt cystic in nature, and was mobile under the skin and to the deep structures. There was no skin discoloration. No dimple or sinus tracts were noted. The patient complained of mild tenderness to palpation. The rest of her exam was unremarkable. Targeted ultrasound of the right neck demonstrated the presence of a slightly lobular 1.1 x 1.1 x 0.5 cm ovoid lesion that appeared to have two fatty hila with central vessels. The lesion was located in the subcutaneous fat. No abnormal tract was seen extending from the area. No fluid collection was seen. The ultrasonographic diagnostic impression suggested a benign bilobed lymph node. Surgical excision of the mass was subsequently scheduled and the specimen was submitted for pathology examination (See Figures 1 to 5).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A term female neonate presented for excision of two prenatally detected oral cavity masses. The pregnancy was uncomplicated, and the neonate was delivered via Caesarean section without complications. Immediately following delivery, the patient was transferred to the operating room. Intra-operative findings included a 1 cm mass of the ventral tongue and a 4 cm mass of the left maxillary alveolar ridge, both of which were excised. At time of discharge, she was feeding orally without issue and was stable on room air.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A woman in her 30's presented with few weeks of productive cough, fatigue, sore throat, and unintentional weight loss. She had been treated for sinus infection and suspected bronchitis with multiple courses of antibiotics. On imaging, she was found to have multiple cavitary lesions in the lung. It was also noted that she had a new bump on her nose. She was admitted and treated with antibiotics for sepsis secondary to suspected pulmonary infection. Over the course of her admission, she developed hypoxic respiratory failure and had multiple episodes of hypotension. Her condition continued to worsen and was pronounced deceased. A hospital autopsy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a female in her 50's who presents for a routine mammography. A density is identified at the 10:00 position in the left breast on craniocaudal (LCC) and mediolateral (LML) views (Figure 1). To further examine this lesion, diagnostic mammography, left breast ultrasound, and a left axillary ultrasound are performed. The ultrasound of the left breast demonstrates an irregular, hypoechoic nodule in the 10:00 region, 2 cm deep to the nipple and measuring 1.8 x 1.3 x 1.1 cm (Figure 2). The diagnostic mammography recapitulates these findings. The left axillary ultrasound shows normal appearing lymph nodes. The nodule is classified as indeterminate by the radiologist and ultrasound-guided biopsy of the lesion is recommended. This was consistent with a BI-RADS category of 4A, denoting a suspicious abnormality. The patient underwent an ultrasound guided biopsy with clip placement at the biopsy site.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A female in her 50's with a known history of neurofibromatosis type 1 since childhood, and a number of previously resected neurofibromas, presented with an enlarging right flank mass concerning for a plexiform neurofibroma. A computed tomography (CT) abdomen and pelvis with contrast demonstrated a cystic mass measuring up to 7.4 cm within the right abdominal wall (Figure 1, A) with areas of calcification and enhancement.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A woman in her 60's, with a past medical history of non-alcoholic cirrhosis, obesity, hypertension, hyperlipidemia, thyroid carcinoma, and poorly controlled type 2 diabetes mellitus presented to the emergency room with headache, nausea, and vomiting. A head computed tomography scan and laboratory studies were normal, and the patient was discharged with migraine medications. The patient returned to the emergency department 4 days following her initial discharge due to multiple falls associated with episodes of loss of consciousness triggered by supination, as well as hallucinations. On examination a hematoma involving her forehead, multiple rib fractures, a right knee laceration and a right patellar fracture we noted, and an EKG showed first degree AV block. Additional workup included blood work which revealed leukocytosis, which prompted blood cultures, in addition to elevated ammonia levels. Due to the patient's altered mental status and intermittent loss of consciousness, an EEG was performed and read as negative. A psychiatry consultation suggested delirium, the cause of which remained unclear. A MRI of the head was ordered but the patient refused. On the morning of the third day after admission, the patient had a cardiac arrest and resuscitation efforts were unsuccessful. An autopsy was requested in an attempt to identify the underlying cause of death.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A woman in her 60s with a history of clear cell endometrial adenocarcinoma status post hysterectomy and chemotherapy, and breast cancer status post lumpectomy and radiation therapy, presented to her primary care physician with left eyelid droop. On physical exam, a nontender mass was palpated in the region of the left parotid. MRI of the brain showed no intracranial abnormality but identified an enhancing nodule in the deep portion of the left parotid gland, for which ENT evaluation was recommended.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a woman in her 60's presenting with a month-long history of altered mental status, expressive aphasia and confusion. The patient has a past medical history significant for an orthotopic liver transplant due to end-stage liver disease secondary to nonalcoholic steatohepatitis four years prior to the current presentation. The patient is currently taking tacrolimus and mycophenolate.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a female in her 70s with a history of papillary thyroid microcarcinoma status post lobectomy who presents with a 2.9 cm mass of the left kidney upper pole. An incidental mass was found on imaging three years ago, initially showing a 2.4 cm nodule with heterogeneous attenuation and enhancement post contrast administration. She denied any symptoms, smoking history, or family history of urological malignancies. Due to the increase in size, the patient elected to undergo a laparoscopic partial nephrectomy of the mass.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a woman is her late 30's with a history of recurrent scalp lesion. She presented to her PCP with a 3-day history of inflamed scalp lesion and an enlarged lymph node. Physical examination revealed erythematous skin breakdown at the crown to the right of the midline, but no drainage expressible. There was a large, tender right posterior auricular lymph node. She was treated with Bactrim DS for suspected scalp cellulitis. One week after her initial presentation, she developed a fever, jaundice, emesis and coca cola-colored urine. She presented to an outside hospital and was transferred to UPMC for further evaluation. On admission, she was hemodynamically stable. Physical examination revealed scleral icterus. Relevant laboratory results are shown below.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.