(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 40-year-old male presented with progressive blurry vision and a restricted peripheral vision. He also described seeing "tiny raindrops" in the frontal vision field.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a gentleman in his 40s with a history of cerebrovascular accident and questionable medication compliance who presented with right-sided weakness and aphasia. Imaging revealed a stroke involving the left middle cerebral artery (MCA) territory for which tissue plasminogen activator (tPA) was administered. Shortly after receiving tPA his weakness worsened and follow-up imaging demonstrated intraparenchymal hemorrhages. A brain MRI performed as part of the stroke workup showed multiple foci of embolic infarcts. A transesophageal echocardiogram revealed aortic insufficiency with calcifications, nodular deposits, and vegetations present on the aortic valve. Blood cultures were obtained and the patient was started on cefepime and vancomycin for presumed endocarditis. Cardiology was consulted and recommended aortic valve replacement to be performed 4-6 weeks following the initial stroke. Blood cultures demonstrated no growth and the patient was maintained on empiric antibiotic treatment until the time of his heart surgery.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 60-70 year old male patient with a history of prostate cancer presented to the ED after being informed that they had abnormal findings on blood work drawn the previous day at their oncology appointment. Lab results showed a hemoglobin of 6.8. The patient denied any symptoms, including fatigue, dizziness, lightheadedness, chest pain or shortness of breath. The patient reported having consistently low hemoglobin values since receiving chemotherapy the previous year. A review of the patient's lab revealed a recent downward trend in the patient's hemoglobin values.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in his 80's who was admitted to our hospital and was being treated for pneumonia, complained of a slow growing, non-healing lesion of unknown duration near his right shoulder. Patient's medical history was significant for atrial fibrillation, and COPD and surgical history was significant for a Basal cell carcinoma on nasal tip. Clinical examination revealed 2.0 cm ulcerated plaque with pink border on the right shoulder (Figure 1) and another pink plaque with crust on the left frontal scalp which measured 1.4 cm in maximum dimension. Considering the patient's past history and clinical presentation of the lesions; basal cell carcinoma was high on differential and both of these lesions were treated with excisional biopsy with electrodessication and curettage and the specimen was sent for histopathological examination.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
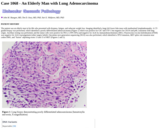
The patient was an elderly man in his 80s who presented with dyspnea, fatigue, and subacute weight loss. Imaging identified a large left lower lobe mass with mediastinal lymphadenopathy. A CT-guided biopsy was performed, which identified a poorly differentiated adenocarcinoma (Figure 1) which was positive for CK7 and TTF-1 but negative for CK5/6 and p40, consistent with lung origin. Ancillary testing was performed, and the tumor cells were positive for PD-L1 (TPS 50%) and negative for ALK by immunohistochemistry (IHC). Fluorescence in-situ hybridization (FISH) was negative for ALK rearrangement (other targets failed). Oncomine next generation sequencing (NGS) was also performed, which identified a TP53 mutation, MET splice site mutation near codon D981, and "fusion" adjoining exons 13 and 15 of MET (Figures 2 and 3).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was an elderly man with history of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), recently started on ibrutinib, who presented with high fever, chills/rigors, night sweats and altered mental status. He was also noted to be hypotensive, which responded to IV NS. His spleen was enlarged, measuring up to 14.6 cm on ultrasound. He had no known significant recent exposures or travel. This occurred in the winter.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 10-month-old boy born by vaginal delivery to non-consanguineous parents (mother G0 P0, 28 years old) after an uneventful term pregnancy (38 weeks and 5 days). There was no in utero exposure to tobacco, illicit drugs or alcohol, and a standard prenatal care schedule was followed. Although early development after birth was normal, the patient was diagnosed with scoliosis at 3 months of age (~25-30 degrees). At 4 months of age, there were episodes where he appeared to stop breathing. Subsequently, at 6 months of age, he lost the ability to lift his head. A Genetics consult identified failure to thrive, weight loss, and gross motor delay. Initial genetic workup included a single nucleotide polymorphism array, fragile X syndrome assessment, and testing for spinal muscular atrophy, all of which were normal. Autism Spectrum Disorder (ASD) and Intellectual Disability (ID) Comprehensive Panel with automatic reflex to whole exome sequencing was performed but was uninformative, identifying only carrier status for recessive disorders.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A previously healthy 44-year-old female presented to the emergency department with sudden onset, bilateral throbbing headaches of two weeks duration. Three days prior to admission, she experienced several episodes of vomiting. Neurological examination was unremarkable and funduscopic examination showed no evidence of papilledema. CT and MRI of the head revealed a partially cystic, hemorrhagic mass with discrete calcifications in the cerebellomedulllary cistern with compression of the midbrain, of the foramina of Luschka bilaterally and of the foramen of Magendie (Figs 1A, 1B, and 1C). The radiographic differential diagnosis favored either subependymoma or medulloblastoma. The patient was admitted to the neurosurgical unit and underwent a craniotomy with gross total tumor resection. Postoperative recovery was unremarkable.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An eighteen month old male with a past medical history significant for febrile seizure presented for a well child visit with parental complaints of fussiness and pallor. On laboratory assessment, he was found to have hemoglobin of 2.4 g/dL with MCV of 79.4 fL and reticulocyte count of 0.3%. The patient was admitted to the hospital and transfused with packed red blood cells. PCR for parvovirus was performed and was negative. One month later, a bone marrow biopsy was performed when the anemia did not resolve. Testing of exons 1-6 of the RPS19 gene associated with Diamond-Blackfan anemia did not identify any disease-associated mutations.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An eight year old boy with a history of autism and cerebral palsy was brought to his pediatrician by his mother for new onset staring episodes. According to the mother, the infrequent episodes are typified by the boy stopping suddenly, staring and becoming unresponsive. The mother also noted that the child has been sleeping more in recent weeks. The child's history is negative for convulsions, myoclonic jerks, meningitis, encephalitis or severe head trauma associated with loss of consciousness.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An elderly gentleman presented with a plaque-like crusted lesion of his right temple in conjunction with supraclavicular lymphadenopathy. The lesion was excised and excisional lymph node biopsy was performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
MRI revealed an irregular 2.0 x 2.5 x 3.0 cm right frontal lobe ring enhancing mass with edema (Figure 1). The lesion was believed to represent a primary or secondary tumor. A resection of the right frontal lobe lesion revealed a gliotic solid and cystic mass. The resected lesion consisted of irregular tan to pink fragments of tissue measuring 3.5 x 1.2 x 0.5 cm.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 12- day old female with who was diagnosed with Downs Syndrome. Her karyotype showed trisomy 21. She was noted to have mild cyanosis with symptoms of mild hypoxemia. Her initial blood count demonstrated severe anemia and thrombocytopenia. Flow cytometry, performed on her peripheral blood showed a >20% population of myeloblasts. A bone marrow smear and aspirate was subsequently ordered. All her other blood work including coagulation studies were normal.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 5 month-old male infant was brought to the Emergency Department by his parents with persistent, worsening shortness of breath, tachypnea and wheezing. The boy was lethargic, anorexic. He had a history of poor sleep, fussiness and crying for two days. No fever, diarrhea, vomiting, drooling, foreign-body ingestion or stridor were noted. No asthma, recent illness or antibiotic ingestion, home treatment, recent infectious exposure or immunizations were recorded. There was evidence of dehydration, with limited tearing and decreased urine output. Oral intake was limited.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
This is a newborn female with trisomy 21 who also had abnormal newborn screening test showing elevation of C5-hydroxy acylcarnitine. Urine organic acid analysis revealed elevation of 3-hydroxyisovaleric acid and 3-methylcrotonylglycine. Further testing included skin biopsy for fibroblast cultures and assay of 3-methylcrotonyl-CoA carboxylase activity that was significantly below the control range (6% of normal).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 3-month-old male infant with pain over the left scrotum for two days. The mother noticed bluish discoloration of the left scrotum and took the patient to the hospital. Ultrasound of the scrotum revealed no flow to the left testis and flow to the right testis. Physical examination revealed hard and enlarged left testis, 2 cm, tender to palpation. The right testis and the penis were normal in appearance. Lab test showed normal AFP level.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 1-year old male (with no significant past medical history) presented to the Department of Plastic Surgery for evaluation and eventual resection of a subcutaneous frontal mass. Imaging of the head revealed a second intracranial mass and he was referred to the Department of Neurosurgery. Subsequently, Magnetic Resonance Imaging (MRI) detected two T-1-hyperintense masses. One was the extra-cranial frontal mass noted clinically and the other was an intra-axial, interhemispheric frontal mass. Additionally, partial agenesis of posterior corpus callosum was found. (Figure 1) At that time, only the subcutaneous mass was resected and physical examination was normal.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
1 year-old male, born at 37 weeks gestation for a gravida 2 para 1 aborta 1 twenty-one year-old female, presented with delayed speech.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
22 y/o Chinese male evaluated in early November with three weeks of gradually worsening edema and lower extremity pain (right >>> left). He reported dry mouth, oral ulcers, non-productive cough, and some stiffness in his hands throughout the day and fatigue. He denied rash, fevers, chills, malaise, weight loss, poor appetite, dry eyes, chest pain, and shortness of breath, nausea/vomiting/diarrhea or changes in urination, raynauds or photosensitivity. He denied any history of tuberculosis or weight loss.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.