(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A pregnant female patient in her early 30s was admitted to hospital with a history of 32 weeks gestation. There were signs of severe fetal suffering and an unusually large fetal skull was detected in ultrasound examination. A cesarean section was performed and a baby girl was delivered with cyanosis, vomiting and irritability. After basic neonatal procedures, neurosurgical evaluation revealed a large skull with congested and prominent superficial vasculature, prominent eyes, and a bulging anterior fontanel with wide open sutures. CT scan showed a large partially cystic mass that occupied approximately half of the intracranial space. Marked hydrocephalus was also noted. A neurosurgical procedure was performed and several fragments of the tumor were submitted for neuropathological examination. The baby expired at age 2 months and an autopsy examination was not performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 47-year old Hispanic male with end-stage AIDS was admitted to the hospital with pneumonia, altered mental status and right-sided weakness. His previous medical history was obscure. He had never received antiretroviral treatment. Upon his arrival he was cachectic, tachycardic and lethargic. His neurologic exam showed left facial palsy, right hemiparesis, hyperreflexia, and a positive right Babinski sign. He had no signs of meningeal irritation. On admission his white blood cell count was 8400/mm3 (98% neutrophils), and his CD4+ cell count was 8 cells/mm3. The serum cryptococcal antigen was negative. IgG and IgM toxoplasma antibodies were positive. A MRI was ordered which was suggestive of neurotoxoplasmosis. He was started on piperacillin-tazobactam, clarithromycin and trimethoprim / sulfamethoxazole for pneumonia, valgancyclovir for skin biopsy proven CMV infection, fluconazol for oral candidiasis and pyrimethamine and clindamycin for toxoplasmosis. Although he continued disoriented and sleepy, he was stable for a few days. On the 18th hospital day he developed severe respiratory distress. He became stuporous and presented right midriasis and ptosis, impaired adduction of the right eye, and generalized seizures. He required immediate ventilatory support and high doses of vasoactive amines. Intravenous amphothericin B infusion was started in order to broaden the antimicrobial coverage, but the patient died five days later.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Magnetic resonance imaging showed widening of the cervical spine with hypointensity on T1 (Fig. 1), increased intradural intramedullary T2 signal (Fig. 2), and contrast enhancement (Fig. 3). The abnormal T2 signal extended from the craniocervical junction to T5, and the abnormal enhancement extended from the craniocervical junction to T3. No abnormalities were seen in the remainder of the brain.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
In the 35th week of gestation a fetal sonography was performed which showed a parietal mass. Anamnestic examination of the African mother revealed a history of minor abdominal trauma. In the 28th week of gestation she had slipped on a wet floor, but had not experienced any subsequent hematoma or vaginal bleeding. She was otherwise well and had no signs of infectious disease; in particular, anti-HIV-antibodies were negative. She had lived in Germany throughout her pregnancy. In the 38th week of gestation the diameter of the parietal mass was about 5 cm. A Caesarian section was performed at this stage. Laboratory investigations were normal, apart from reduced prothrombin time (PT) (Normalized Ratio 0.11; normal range 0.9-1.2) and the mother had no abnormal coagulation. After vitamin K substitution and application of fresh frozen plasma, the PT was within normal range. No jaundice or swelling of lymph nodes was observed. Both the neonate and his mother had the identical blood group, B positive. No macroscopic abnormalities of the placenta or umbilical cord were observed. The entire mass was removed at surgery. Postoperatively, the boy recovered well. Neurological examination showed slightly reduced spontaneous movement of the right side. Two weeks later, both mother and son were discharged from hospital.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 53-year-old female with an enlarging mass in the right lower quadrant.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 45 y/o caucasian male with no significant past medical history who was well until May of 2007. He works as a machinist and at that time had a small wire penetrate the thenar eminence of his right hand. For several days he had a small amount of purulent drainage which resolved spontaneously. In June of 2007 his right 2nd finger became swollen and he was prescribed a 5 day course of Prednisone that provided temporary improvement followed by injections into the 2nd and 4th metacarpal joints and the wrist when the swelling returned.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
In October 2008, a 72-year-old man was referred to us with a three week history of dizziness and unsteady gait.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 12-year-old male was admitted to our hospital complaining of right upper limb tremor, loss of the normal capacity to modulate fine voluntary movements with his right hand and headache, lasting for over a month. On neurological examination dysdiadochokinesia and intention tremor of the right upper limb was noted. A computed tomography (CT) scan was performed and revealed a large lesion expanding in the right cerebellar hemisphere, compressing the fourth ventricle which was occluded. Magnetic resonance imaging (MRI) of the brain demonstrated the same space-occupying lesion in the fourth ventricle measuring approximately 4 × 3.8 × 4 cm. It was hypointense on T1-weighted images (Fig.1), medium intense on T2 and FLAIR sequences, and heterogeneously enhanced after gadolinium administration (Fig. 2). The lesion was surrounded by edema and caused displacement of the cerebellar vermis and pons. A suboccipital midline craniotomy was performed, the cerebellar vermis was split and the lesion was totally excised.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 2-year-old girl was admitted to the department of neurosciences, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia, with three weeks history of deterioration of walking, then became unable to walk and later she developed a projectile vomiting mostly in early morning. There was no history of seizures or loss of consciousness. At admission her neurological examination revealed bilateral papilledema, nystagmus and truncal ataxia with intention tremor. Magnetic Resonance Images (MRI) of the brain showed a 3x4 cm posterior fossa enhancing mass extending from the base of the cerebellum to the roof of the fourth ventricle without calcification (Figure. 1, sagittal T-1 weighted with contrast) and (Figure 2: axial T2-weighted with contrast). Then, the patient underwent midline suboccipital craniotomy with a near total resection of the tumor.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
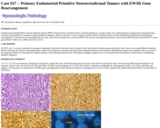
Ewing Sarcoma (ES)/Primitive Neuroectodermal Tumors (PNET) rarely present as primary tumors of female genital tract. In gynecologic tract, demonstration of translocation involving Ewing Sarcoma Gene (EWSR1) is considered a gold standard for diagnosis. Here we describe 2 cases of primary uterine PNETs with Fluorescence in Situ Hybridization (FISH) proven EWSR gene rearrangement. To the best of our knowledge there are only 4 previously reported cases of uterine PNET with reverse transcription polymerase chain reaction (RT-PCR) proven EWSR-FLI1 fusion gene product (Sinkre et al, 2000, Katuria et al, 2011).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
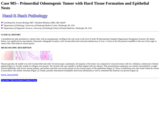
A preadolescent male presented to a dental clinic with an asymptomatic swelling in the oral cavity at the level of tooth 38 (International Standard Organization Designation System). His dental history was significant for macrodontia. Panoramic radiograph revealed a well circumscribed and corticated radiolucency (2.2cm x 2.0cm) of the left posterior mandible in the area of the angle to ramus with a faint band of central opacity.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An 8-year-old boy with no significant past medical history presented to the emergency department following 2 weeks of progressive headaches, fatigue, and vomiting. On physical examination, the patient had no fever, or focal motor or sensory neurological deficits. Initially diagnosed with an H1N1 viral upper respiratory and gastrointestinal infection, he was discharged home with conservative management. After failure to improve over the next several days, a superimposed bacterial infection was suspected. He was given a course of oral antibiotics, which failed to improve his symptoms. Imaging revealed a large, heterogenously enhancing mass measuring 5.6 x 4.7 x 5.2 cm, which contained partially hemorrhagic material centered within the left thalamus extending into the body of the lateral ventricle (Figures 1, 2, 3, 4). Gross total resection of the tumor was confirmed by postoperative imaging. Staging revealed no metastases. The patient was discharged home 1 week later.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 31 year-old female that moved to Pittsburgh from California one year back. She has a history of episodic pain involving arms, legs and abdomen (pain usually starts at night or in the morning when she wakes up). In July of 2008 she developed pain crisis at child delivery. After her move to Pittsburgh, in May 2009, she was admitted to a hospital with nausea and vomiting. A CT scan was consistent with pneumonia. She had a favourable course after being treated wih Azithromycin. Three months later, in August 2009 she presented to the same hospital complaining of fever and productive cough (green sputum). Once again, her diagnosis was pneumonia and she improved after iv Moxifloxacin. Her clinical scenario prompted an extensive work-up, including a CBC and peripheral blood smear.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 31 year-old male, status post-kidney transplant three years ago, who presented with increased creatinine. The patient was seen in an outside hospital and the biopsy was submitted to UPMC for consultation.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 19 year-old female with no significant medical history who presented with a palpable, tender nodule in her left axilla and left-sided rib pain. The patient denied headache, fevers, chills, night sweats, and recent weight loss. She also denied sick contacts, shortness of breath, and recent bruising or bleeding.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
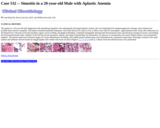
The patient is a 20-year-old male diagnosed with autoimmune hepatitis who subsequently developed aplastic anemia. He was hospitalized for immunosuppressive therapy and evaluation for possible bone marrow transplant. The patient remained markedly leukopenic with white blood cell counts as low as 200/cu mm with 4% neutrophils. Approximately three weeks after admission, he developed fever with pain in the left maxillary region, facial swelling, and gingival bleeding. Computed tomography demonstrated left paranasal sinus opacification, periapical lucency surrounding the left premolar/molar teeth, cellulitis of the left buccal and masseteric regions, and subtle retromaxillary fat obscuration. No abscess or osteomyelitis was noted. Blood cultures were persistently negative. The patient underwent sinonasal surgery for tissue debridement, including a left middle partial turbinectomy, total ethmoidectomy, and partial septectomy. Histologic sections of the nasal septum and turbinate showed numerous fungal hyphae and conidia with tissue invasion [Figures 1, 2, 3, 4, 5, 6 and 7]. Cultures from the turbinate tissue were performed.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 58- year-old man with clinical diagnosis of phacomatosis pigmentovascularis (PPV) was admitted to our neurosurgical department with a 5-year history of tinnitus, progressive hearing loss on the right and headaches. On physical examination, multiple melanocytic and vascular nevi (more than150) together with 20 atypical nevi, extensive port-wine stains on the first and third divisions of the trigeminal nerve, and blue spots over his right shoulder, neck, head, ear and face were identified (Figure 1). No ocular pigmentation, increased ocular pressure or seizures were observed. On neurological evaluation, only hearing loss was found.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
This was a 62 years old gentleman with a medical history of single right lung transplant for idiopathic pulmonary fibrosis. Post transplant cultures showed heavy Staphylococcus aureus (S.aureus) and he was treated with IV Vancomycin for 10 days. The first surveillance bronchoscopy with biopsy was negative for organisms or rejection and the patient was discharged.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Acute myeloid leukemia (AML) is a highly aggressive and extensively studied hematological malignancy which is known to affect around 13000 adults in United States annually (1). Cytogenetic aberrations are the most important diagnostic and prognostic findings in patients with AML, however karyotype abnormalities are identified in only half of all AML cases (2, 3). Cryptic rearrangements involving the lysine (K)-specific methyltransferase 2A (KMT2A) has been detected in ~ 5-10% cases of adult patients with cytogenetically normal AML (4, 5). The KMT2A gene, located at 11q23, is involved in a number of the translocations with more than 90 gene partners. Many of these rearrangements can be detected by karyotype or by fluorescence in situ hybridization (FISH) studies using KMT2A break apart probe. A partial tandem duplication (PTD) in the KMT2A gene is a cryptic alteration, undetectable by either karyotype or FISH, and produces an in-frame, elongated protein (6). We present a case of AML with normal cytogenetic results, in which a KMT2A-PTD was detected by microarray analysis.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a man in his 70s who presented with an isolated thyroid nodule in the right mid-lower pole. He subsequently underwent fine needle aspiration, and specimens were submitted for cytology interpretation and molecular testing.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.