This narrated slide show gives a brief overview of coral biology and …
This narrated slide show gives a brief overview of coral biology and how coral reefs are in danger from pollution, ocean temperature change, ocean acidification, and climate change. In addition, scientists discuss how taking cores from corals yields information on past changes in ocean temperature.
Open science describes the movement of making any research artefact available to …
Open science describes the movement of making any research artefact available to the public and includes, but is not limited to, open access, open data, and open source. While open science is becoming generally accepted as a norm in other scientific disciplines, in software engineering, we are still strugglingin adapting open science to the particularities of our discipline, rendering progress in our scientific community cumbersome. In this chapter, we reflect upon the essentials in open science for software engineering including what open science is, why we should engage in it, and how we should do it. We particularly draw from our experiences made as conference chairs implementing open science initiatives and as researchers actively engaging in open science to critically discuss challenges and pitfalls, and to address more advanced topics such as how and under which conditions to share preprints, what infrastructure and licence model to cover, or how do it within the limitations of different reviewing models, such as double-blind reviewing. Our hope is to help establishing a common ground and to contribute to make open science a norm also in software engineering.
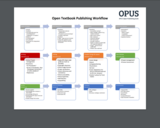
The KPU Open Publishing Suite team has established an Open Textbook Publishing …
The KPU Open Publishing Suite team has established an Open Textbook Publishing Workflow v 4.0 that is used to ensure the project moves from beginning to end smoothly. It will show you the different stages that a project moves through, and which questions and items to consider at each stage.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 34 year-old otherwise healthy man presented with new onset headaches, mild confusion, and subtle left-sided weakness. An MRI scan showed a large heterogeneous 8.9cm x 6.0cm right fronto-temporo-parietal mass with nodular enhancement, significant surrounding edema, and 15mm of midline shift. He underwent an urgent right craniotomy, and began appropriate therapy. Unfortunately, within one week of completion of this therapeutic regimen, his symptoms worsened. He was found to have multiple new bilateral dural-based nodular enhancing lesions on repeat brain MRI. No spinal abnormalities were found. He underwent resection of one of the new lesions. The patient was initiated on a new treatment plan, but unfortunately, neuroimaging revealed further progression of disease (Figure 1). He passed away 5 months and 1 day after diagnosis.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient was a 35-year-old African American woman with HIV/AIDS (CD4 count 95/ml) and no history of HAART therapy, who was admitted from an outside hospital for further management of altered mental status and hypercarbic respiratory failure. Upon admission, the patient was unresponsive and ventilator dependent. On neurologic exam she had no response to painful stimuli, as well as decreased deep tendon and pupillary reflexes. A chest X-ray failed to demonstrate any pulmonary lesions. A CT of the head without IV contrast revealed an infiltrating hypodense mass within the basal forebrain extending inferiorly to the level of the basilar cisterns, involving the thalami and cerebral peduncles bilaterally (Figure 1). Diffuse brain volume loss was also noted. A lumbar puncture was performed for CSF analysis, which showed lymphocytic pleocytosis (56 nucleated cells/ml with 92% lymphocytes), low glucose (23 mg/dl) and elevated protein (208 mg/dl). An infectious disease was suspected. PCR analysis of the CSF was negative for Mycobacterium tuberculosis, HSV, VZV, CMV and JC virus. There was low positivity for EBV DNA. Serologic studies were consistent with past infections with EBV and CMV and were negative for toxoplasmosis, histoplasmosis, Cryptococcus and West Nile virus. VDRL was non-reactive. CSF and blood cultures for bacteria, fungal organisms and acid fast bacilli were negative. The patient received empiric therapy for bacterial meningitis, including Mycobacterium tuberculosis, HSV/VZV encephalitis and coverage for fungi with amphotericin. Her neurologic status progressively deteriorated. She lost all deep tendon reflexes and her left pupil became fixed and dilated. The presence of corneal reflexes was the only sign of remaining brain stem function. The decision to end life sustaining treatment was made and the patient expired. Consent for limited autopsy of the brain was obtained from the family.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 45-year-old man presented to us with headache and vomiting for15 years ago. He was diagnosed as having obstructive hydrocephalus due to a pineal region tumour. A ventriculoperitoneal shunt was inserted to relieve hydrocephalus with symptomatic relief. He was followed up with regular MRI scans. Serial imaging showed slow progression in tumor size when he was 60 years old. Neurological examination revealed Parinaud sign with upward gaze palsy. The MRI with gadolinium showed an mildly enhancing lobulated tumor in the region of the superior tectum measuring 22.5mm x 21mm x 20mm (Figs. 1 and 2). The lesion at the superior tectum and the pineal region showed heterogeneous T1-hyperintense signal on precontrast images (Fig. 1). It exhibited very slow growth, with a gradual increase in size over 15 years. There was mild mass effect to the cerebral aqueduct with indentation of the pineal gland (Fig. 3). However, there was no hydrocephalus at that time. In view of symptomatic progression of tumor size, he underwent a near total tumour excision via infratentorial supracerebellar approach.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 66-year-old female with metastatic colon cancer presents to the emergency department with the complaint of weakness, which was so bad that she had to be carried to the car before being driven to the ED. She underwent debulking surgery one month prior to presentation and has since followed up for problems including fecal impaction and diarrhea. She has poor oral intake and is losing weight. She reports compliance with her bowel regimen of docusate sodium, senna, polyethylene glycol, and milk of magnesia. Initial laboratory findings are listed in the table.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 70 year old former farmer and cattle breeder was admitted to a district hospital due to intermittent confusion, neuropsy-chological slowing with otherwise unremarkable neurological examination. His family first noticed personality changes after a right knee arthroscopy two weeks earlier.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 72-year-old woman presented with a 4-year clinical history of increasing confusion, memory loss, depression, and dizziness. Neuroimaging studies including CT and MRI showed bifrontal dural masses (Figure 1a) and a right-sided tentorial mass in the cerebello-pontine angle (Figure 1b). The supratentorial masses were considered suspicious for multiple meningiomas or CNS lymphoma, whereas schwannoma was favored for the cerebello-pontine angle mass. Microsurgical resection was performed of the both frontal lesions and right cerebello-pontine mass. After the pathological diagnosis was rendered, systemic lesions were detected by PET in the humerus and femur, piriform sinus, ilium, clavicles and mandible (Figure 1c). The patient underwent a course of vemurafenib treatment, a BRAF-inhibitor, which improved the neurological status.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A 3 month previously healthy female with no significant family history presented with a 2 day history of fever (38.8 °C) abdominal distention and tachypnea. Initial laboratory evaluation demonstrated pancytopenia with absolute neutropenia, elevated liver function tests, prolonged coagulation times, hyperlactatemia and elevated ferritin levels (Table 1). An infectious workup was negative (EBV, CMV, Adenovirus, Influenza, Parainfluenza, RSV, Chlamydia, Mycoplasma, Anaplasma and all cultures). A bone marrow biopsy was performed and demonstrated histiocytes with hemophagocytosis (Figure 1). Further testing demonstrated elevated soluble IL-2 receptor levels (>20000 pg/mL (Reference range: 622 to 1619 pg/mL). Subsequently genetic testing ordered was positive for biallelic mutations in PRF1.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a 54-year-old female presenting with shortness of breath, malaise, and cough.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a female in her 60s who presents with an incidentally detected kidney mass. Computed tomography shows an enhancing 2.0 cm exophytic, solid right kidney mass of the lower pole. She denies any symptoms, smoking history, or family history of urological malignancies. The patient elects to undergo a laparoscopic partial nephrectomy of the mass in lieu of continued surveillance.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a premature infant male who was born to a multiparous mother. Early in the mother's pregnancy, routine prenatal screening identified fetal anemia requiring multiple percutaneous umbilical blood sampling (PUBS) procedures and fetal transfusions. A workup for immune mediated causes of fetal anemia was completely negative. During one PUBS procedure, the fetus showed a significant cardiac deceleration, leading to an emergent C-section. His immediate post-delivery course was complicated by multiple prematurity associated comorbidities, as well as unexplained persistent anemia without reticulocytosis requiring transfusion support. Hematology was consulted for the persistent anemia and recommended a bone marrow aspirate and biopsy.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
The patient is a female in her 70s with a history of papillary thyroid microcarcinoma status post lobectomy who presents with a 2.9 cm mass of the left kidney upper pole. An incidental mass was found on imaging three years ago, initially showing a 2.4 cm nodule with heterogeneous attenuation and enhancement post contrast administration. She denied any symptoms, smoking history, or family history of urological malignancies. Due to the increase in size, the patient elected to undergo a laparoscopic partial nephrectomy of the mass.
(This case study was added to OER Commons as one of a …
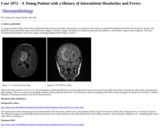
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A young previously healthy child with no significant medical history presented to their primary care physician with a history of intermittent headaches and fevers for the past few months. The headaches had no predictable pattern and no positional triggers or intensity change. The patient was initially treated with oral antibiotics, which failed to improve their symptoms. They then developed gait disturbances and visual changes, prompting imaging studies (Figures 1 and 2).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A man in the seventh decade of life lives independently and has end stage liver disease. He presented to the ED with complaints of increasing gait disturbances over the past several weeks and new onset diplopia and blurry vision. He also complains of persistent headaches, body aches, and intermittent confusion. He had nausea and vomiting, which had impaired his ability to take his lactulose as prescribed. Recently, he had been admitted to the hospital multiple times for what was diagnosed as hepatic encephalopathy. The patient was admitted to the hospital and neurology was consulted.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
An 81 year-old female presented to the emergency department with complaints of blood in her urine and stool for 1 day and new onset of weakness. She has a history of congestive heart failure, type 2 diabetes, and nonalcoholic steatohepatitis. She had a cough one week ago. At presentation she appeared jaundiced. The patient had no recent blood transfusions. Relevant laboratory values (Table 1) and blood bank test results (Table 2) are reported below.
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
Her initial physical exam in the emergency department revealed a distended, non-tender lower abdomen with a large palpable midline mass. The remainder of her physical exam was unremarkable. Initial laboratory workup was unremarkable, including normal levels AFP, hCG, LDH, CEA-125, and estriol. She underwent ultrasound of the abdomen and CT scan of the chest, abdomen, and pelvis (Figure 1). The CT scan revealed a solid, enhancing, 19 x 12 x 10 cm multilobulated mass arising from the left aspect of the uterus. This mass distorted the endometrial cavity and exerted significant mass effect on the iliac veins, iliac arteries, and distal ureters. The remainder of the abdominal and thoracic CT was unremarkable. The initial interpretation was worrisome for uterine malignancy, such as leiomyosarcoma or other uterine sarcomas. There was also some concern, based on the combined interpretation of the CT and ultrasound, that the mass could be arising from one or both ovaries. After discussion with the patient and her family of the above findings, and because the patient was clinically stable, she was discharged to home with short interval follow-up. A subsequent MRI of the abdomen and pelvis two days later as an outpatient showed normal appearing ovaries and re-demonstrated the large uterine mass (Figure 2).
(This case study was added to OER Commons as one of a …
(This case study was added to OER Commons as one of a batch of over 700. It has relevant information which may include medical imagery, lab results, and history where relevant. A link to the final diagnosis can be found at the end of the case study for review. The first paragraph of the case study -- typically, but not always the clinical presentation -- is provided below.)
A woman in her 20s presented with a one-year history of bifrontal headaches that had recently worsened. After admission to the hospital, the patient displayed no other symptoms and no acute worsening of the headaches.
No restrictions on your remixing, redistributing, or making derivative works. Give credit to the author, as required.
Your remixing, redistributing, or making derivatives works comes with some restrictions, including how it is shared.
Your redistributing comes with some restrictions. Do not remix or make derivative works.
Most restrictive license type. Prohibits most uses, sharing, and any changes.
Copyrighted materials, available under Fair Use and the TEACH Act for US-based educators, or other custom arrangements. Go to the resource provider to see their individual restrictions.